I have FINALLY obtained an unofficial document that appears to be an updated version of the negotiating text of the proposed amendments to the International Health Regulations.
Please watch the video below…
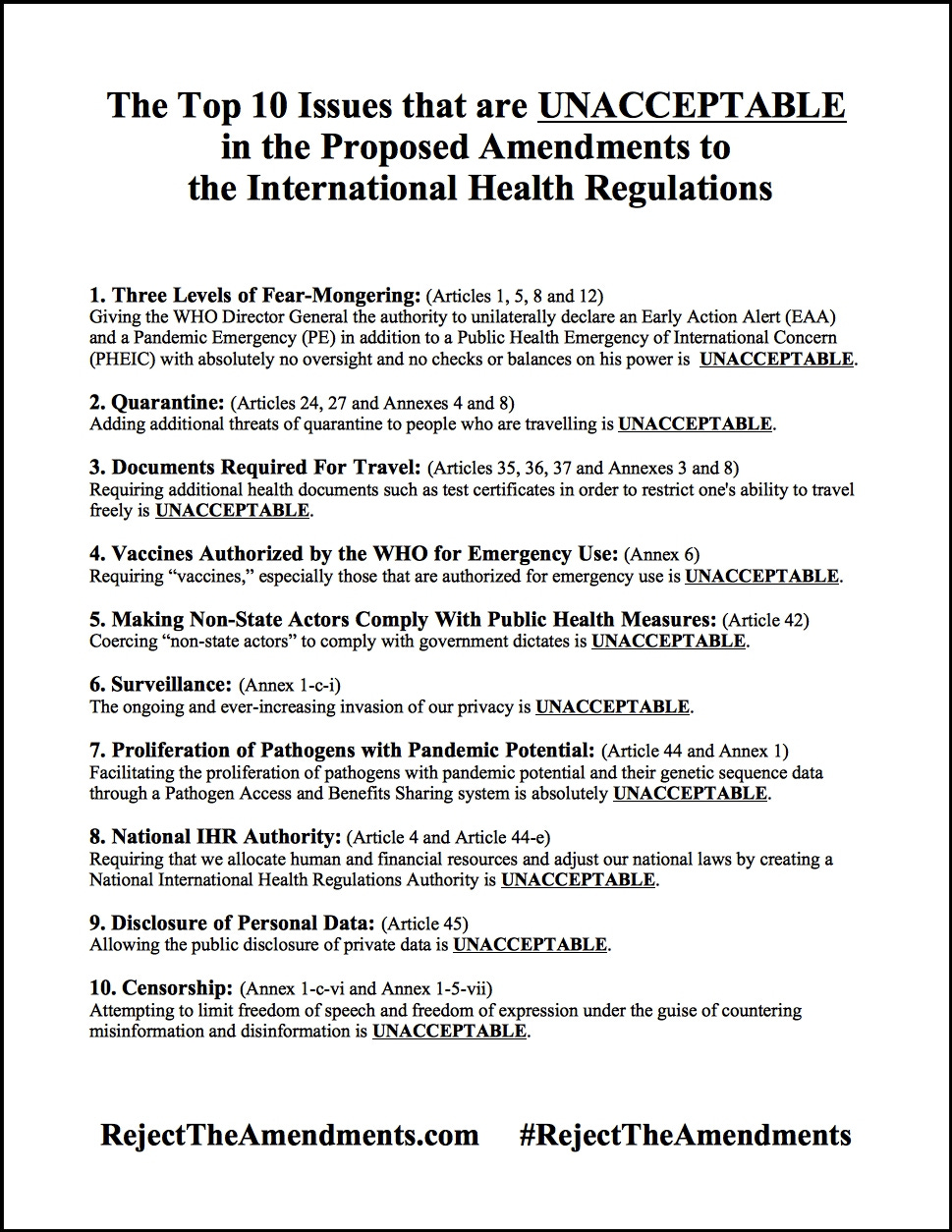
Please download the graphic above by clicking on it and saving it to your phone or computer. Share it far and wide across social media.
You can also download the PDF below, print it out and share it far and wide in the physical world.
Below is a 13-page summary of proposed amendments to 18 articles and 5 annexes of the International Health Regulations.
Scroll down for the text version.
Regular text below is from the IHR(2005).
Bold text below is proposed additional amendments.
Struck through text below is text to be deleted.
Article 1: Definitions
“early action alert” means an alert on an event which has not been declared a public health emergency of international concern, at the time of communication
- to potentially require coordinated international action to control spread because the event has a potentially significant localized acute public health impact in a limited number of countries and:
- to constitute a potential risk of international spread and becoming a PHEIC.
“public health emergency of international concern” means an extraordinary event which is determined, as provided in these Regulations:
(i) to constitute a public health risk to other States through the international spread of disease and
(ii) to potentially require a coordinated international response;
“pandemic emergency” means a public health emergency of international concern, that is infectious in nature, in relation to which it is determined, in accordance with Article 12, that the event:
(i) is significantly impacting or is likely to significantly impact various geographic regions around the globe; and:
(ii) is causing or is likely to cause substantial disruptions to social, economic, and health systems, including to travel and trade; and
(iii) requires rapid and enhanced coordinated international action, with global equity based and whole-of-society approaches because the event has continued to spread despite established public health interventions.
Article 4: Responsible Authorities
1. Each State Party shall designate or establish one or two entities, in accordance with its national law and context, to serve as National IHR Authority and National IHR Focal Point, as well as the authorities responsible within its respective jurisdiction for the implementation of health measures under these Regulations.
1. bis The National IHR Authority shall coordinate the implementation of these Regulations within the territory of the State Party.
2. bis States Parties shall take measures to implement paragraphs 1, 1. bis, and 2 of this Article, including, as necessary, by allocating human and financial resources and adjusting their national law, domestic legislative and administrative arrangements in accordance with paragraph 3 of Article 59.
Article 5: Surveillance
3. State Parties with more resources shall make available additional resources to WHO for assisting developing countries to develop, strengthen and maintain the capacities.
5. WHO should develop a early warning criteria for assessing and progressively updating the national, regional, or global risk posed by an event of known or unknown causes or sources and shall convey this risk assessment to states parties in accordance with Article 11 & 45 where appropriate.
Article 8: Consultation
In the case of events occurring within its territory not requiring notification as provided in Article 6, in particular including those events for which there is insufficient information available to complete the decision instrument in order to assess the event within 48 hours in accordance with paragraph 6(a) of Annex 1, a State Party is strongly encouraged to nevertheless consider, whenever appropriate, keeping WHO advised thereof in a timely manner through the National IHR Focal Point and consult with WHO on appropriate health measures within 72 hours of the event being reported. Such communications shall be treated in accordance with paragraphs 2 to 4 of Article 11. The State Party in whose territory the event has occurred may request WHO assistance to assess any epidemiological evidence obtained by that State Party.
Article 12: Determination of an early action alert, a public health emergency of international concern and a pandemic emergency
1. The Director-General shall determine, on the basis of the information received, in particular from the States Parties within whose territory an event is occurring, whether an event calls for an early action alert or constitutes a public health emergency of international concern, including, when appropriate, a pandemic emergency, in accordance with the criteria and the procedure set out in these Regulations.
New 5. The Director-General shall also determine whether a public health emergency of international concern also constitutes a pandemic emergency.
Article 13: Public health response
1. Developed country State Parties and WHO undertake to provide resources to developing countries for the building of capacities pursuant to this provision equivalent to the amount of resources they provided to build capacities under Article 5.
5. When requested by WHO, States Parties shall should provide, to the extent possible, support to WHO-coordinated response activities, including supply of health products and technologies, especially diagnostics and other devices, personal protective equipment, therapeutics, and vaccines, for effective response to PHEIC occurring in another State Party’s jurisdiction and/or territory, capacity building for the incident management systems as well as for rapid response teams. Any State Party unable to fulfill such requests shall inform the reasons for the same to WHO and the Director General shall include the same in the report submitted to WHA under Article 54 of these Regulations.
Article 15: Temporary recommendations
2bis. When communicating the issuance, modification or extension of temporary recommendations, the Director-General shall endeavor to adopt measures and provide information to States Parties on access to, and availability of health products, technologies and know-how through WHO-coordinated mechanisms for fair and equitable access.
Article 16: Standing Recommendations
2. When communicating the issuance, modification or extension of standing recommendations, the Director-General shall endeavor to adopt measures and provide information to States Parties on access to, and availability of, health products, technologies and know-how through WHO-coordinated mechanisms for fair and equitable access.
Article 17: Criteria for recommendations
When issuing, modifying or terminating temporary or standing recommendations, the Director-General shall consider:
h) the availability of relevant health products, technologies and know-how, including in the context of WHO-coordinated access and allocation mechanisms for a fair and equitable access.
Article 24: Conveyance operators
1. States Parties shall take all practicable measures consistent with these Regulations to ensure that conveyance operators:
(a) comply with the health measures which may include isolation and quarantine recommended by WHO and adopted by the State Party including for application on board as well as during embarkation and disembarkation; Such measures, including isolation and quarantine, shall be based on available evidence;
(b) inform travelers of the health measures recommended by WHO and adopted by the State Party including for application on board as well as during embarkation and disembarkation;
[From the International Health Regulations (2005)
“conveyance” means an aircraft, ship, train, road vehicle or other means of transport on an international voyage;
“conveyance operator” means a natural or legal person in charge of a conveyance or their agent;]
Article 27: Affected conveyances
The competent authority may implement additional health measures, including isolation and quarantine of the conveyances, as necessary, to prevent the spread of disease.
Article 35: General Rule
2. Health documents under these Regulations may be issued on non-digital, digital or any other possible format, subject to the obligations of any State Party regarding the format of such documents deriving from other international agreements.
3. Regardless of the format in which relevant health documents under these Regulations have been issued, each State Party shall accept health documents issued by other States Parties, as long as the health documents conform to the Annexes referred to in Articles 36 to 39 and their authenticity can be ascertained.
4. WHO, in consultation with States Parties, shall develop and update, as necessary, technical guidance, including specifications or standards related to the issuance and ascertainment of authenticity of health documents in digital format, as well as non-digital format. Such specifications or standards shall be in accordance with Article 45 regarding treatment of personal data, and supporting the progressive achievement of the interoperability of information technology platforms.
Article 36: Certificates of vaccination or other prophylaxis
3. In accordance with Article 35, other types of proofs and certificates, such as test certificates, issued in conformity with Annex XXX, may be considered by States Parties when accepting the entry of travelers into their territories, in particular when a vaccine or prophylaxis has not yet been made available for a disease in respect to which a public health emergency of international concern has been declared.
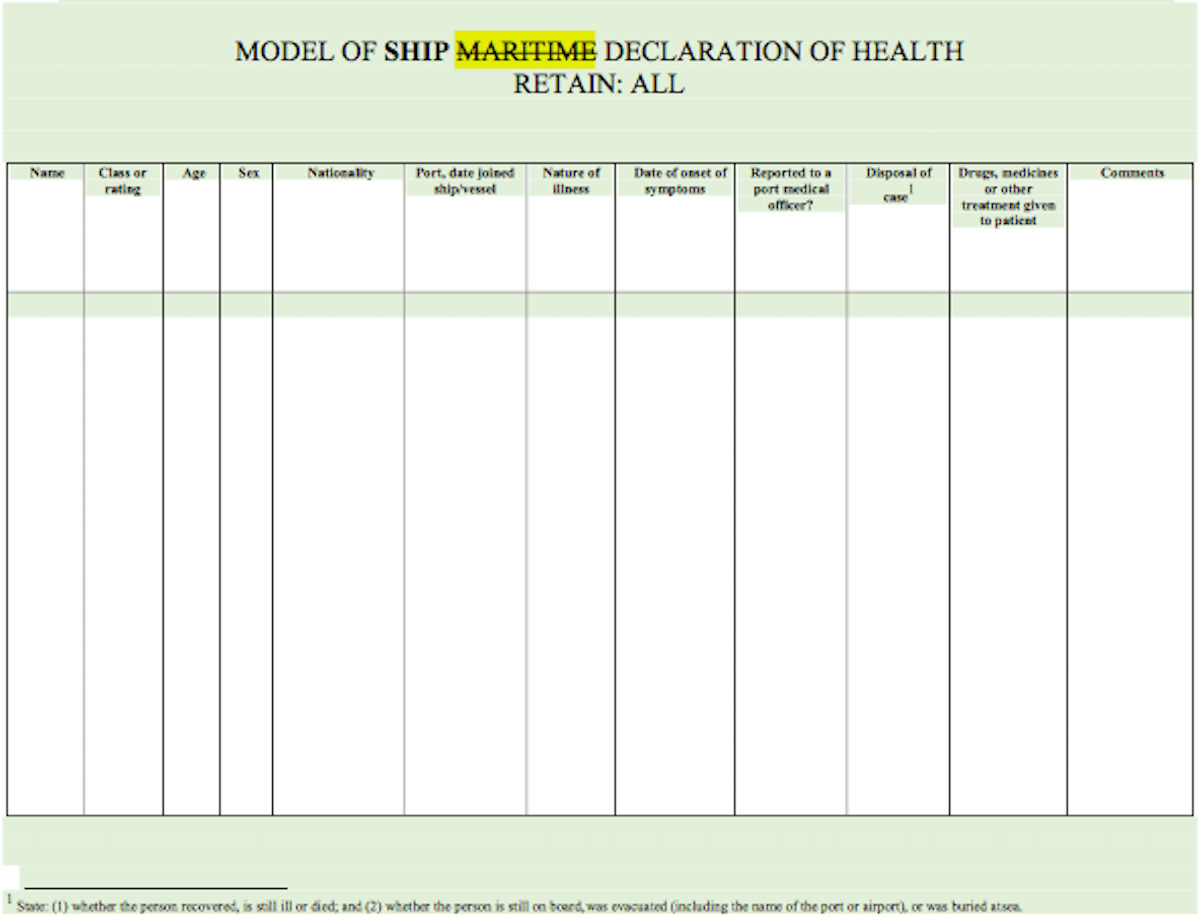
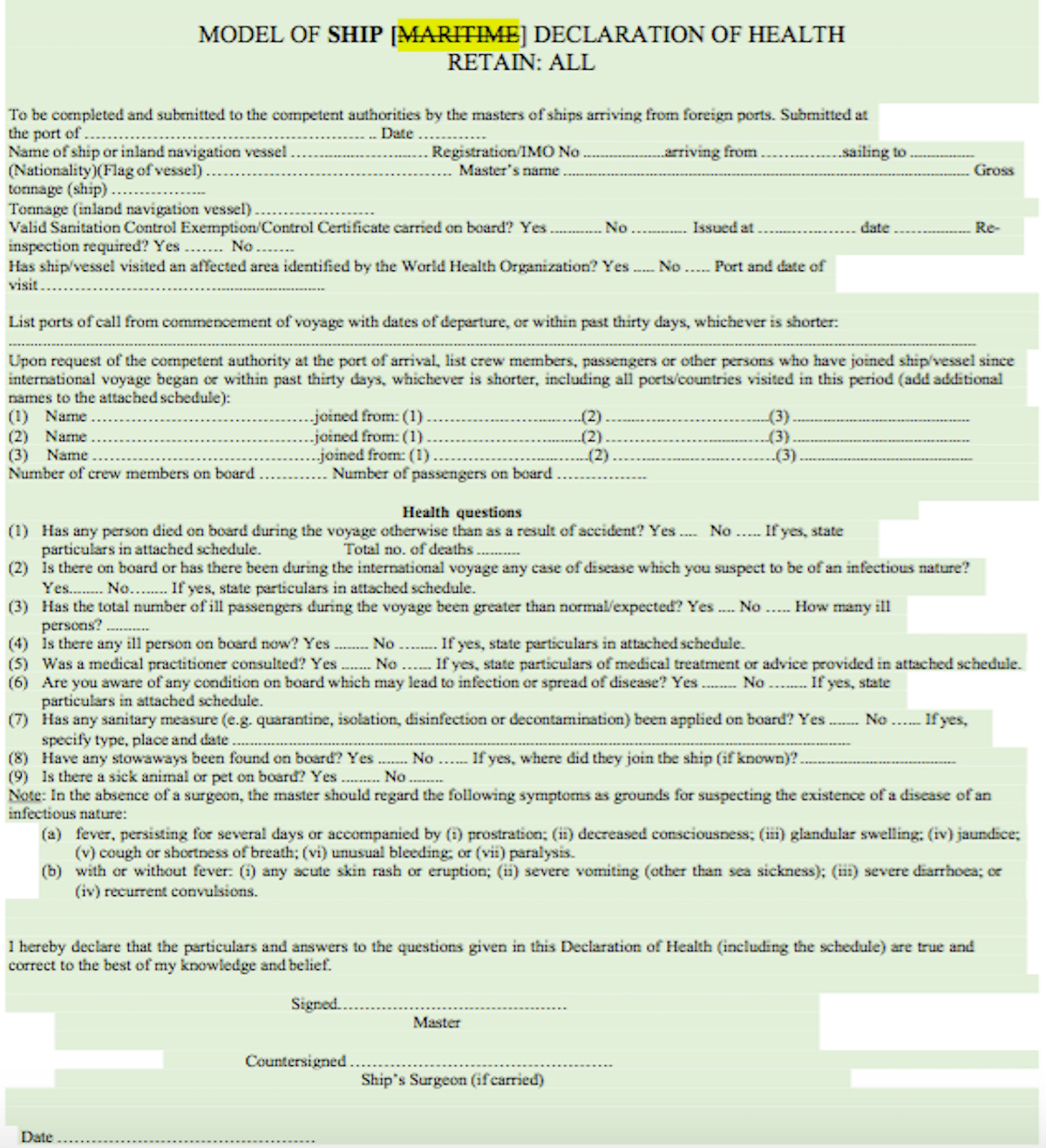
Article 37: Ship Maritime Declaration of Health
1. The master of a ship, before arrival at its first port of call in the territory of a State Party, shall ascertain the state of health on board, and, except when that State Party does not require it, the master shall, on arrival, or in advance of the vessel’s arrival if the vessel is so equipped and the State Party requires such advance delivery, complete and deliver to the competent authority for that port a Ship Maritime Declaration of Health which shall be countersigned by the ship’s surgeon, if one is carried.
2. The master of a ship, or the ship’s surgeon if one is carried, shall supply any information required by the competent authority as to health conditions on board during an international voyage.
3. A Ship Maritime Declaration of Health shall conform to the model provided in Annex 8.
4. A State Party may decide:
(a) to dispense with the submission of the Ship Maritime Declaration of Health by all arriving ships; or
(b) to require the submission of the Ship Maritime Declaration of Health under a recommendation concerning ships arriving from affected areas or to require it from ships which might otherwise carry infection or contamination.
The State Party shall inform shipping operators or their agents of these requirements.
Article 42: Implementation of health measures
State Parties shall take all practicable measures, consistent with relevant national law and their international obligations, to ensure that non-State actors operating in their respective jurisdictions comply with and implement health measures taken pursuant to these Regulations.
Article 43: Additional health measures
3 bis. When implementing additional health measures referred to in paragraph 1 of this article, States Parties shall take all practicable measures to avoid interference with and facilitate unhindered and equitable access to health products required for responding to a public health risk or a public health emergency of international concern.
Article 44: Collaboration and assistance
1. Upon request of a State Party and/or of WHO, States Parties shall, to the extent possible, undertake to collaborate with, and assist each other, in particular developing countries, to the extent possible, in:
(a) the detection and assessment of, and response to, events as provided under these Regulations, including by exchanging, samples and genetic sequence data of pathogens through an equitable and fair ABS system established under the World Health Organization.
(e) facilitating unhindered and equitable access to health products, technologies and know-how through WHO-coordinated mechanisms.
2. WHO shall collaborate with, and assist States Parties, upon request, to the extent possible, in:
(d) facilitating the exchange of samples and genetic sequence data of pathogens through an equitable and fair ABS system established under the World Health Organization.
(e) the formulation of proposed laws and other legal and administrative provisions for the implementation of these Regulations;
(f) facilitating unhindered and equitable access to health products, technologies and know-how, through WHO-coordinated mechanisms.
Article 45: Treatment of personal data
2. In the event that processing or disclosure of personal data pursuant to this paragraph would result in public disclosure of such personal data, the State Party concerned shall inform, if possible prior to such public disclosure, the State Party that provided the data.
ANNEX 1: CORE CAPACITY REQUIREMENTS
1. States Parties shall take specific measures to strengthen broader health systems capacities, such as primary health care and hospital care facilities, while investing domestically and providing international assistance for building capacities under this Annex.
New 4. State(s) whose existing/ and or strengthened national structures and resources are not able to meet the core capacity requirements within time frame stipulated under para 2, shall be supported by WHO to fill gaps in critical capacities for surveillance, reporting, notification, verification, response.
At the local community level and/or primary public health response level (hereinafter the “Local Level”)
Each State Party shall develop, strengthen and maintain,
The capacities:
(c) to coordinate with and support the local level in preparing for and responding to public health risks and other events, including in relation to:
(i) surveillance;
(ii) on-site investigations, including multidisciplinary and /or multisectoral;
(iii) laboratory diagnostics, including referral of samples and genetic sequencing;
(iv) implementation of control measures;
(v) provision of access to health services and relevant health products;
(vi) risk communication, including countering misinformation and disinformation; and
(vi bis) provision of health information system to support emergency operations
(vii) provision of logistical assistance.
5. At the national level
Public health preparedness and response. The capacities:
(a) to coordinate with and support the local and intermediate levels in preparing for and responding to public health risks and other events, including in relation to:
(ii) collaborative / multi-sectoral, multidisciplinary surveillance;
(vii) risk communication, including countering misinformation and disinformation;
B. CORE CAPACITIES REQUIREMENTS FOR DESIGNATED AIRPORTS, PORTS AND
GROUND CROSSINGS
1. At all times
The capacities:
(pre a) to establish surveillance at Points of Entry.
(c) to provide trained Point of Entry workforce personnel for the inspection of conveyances;
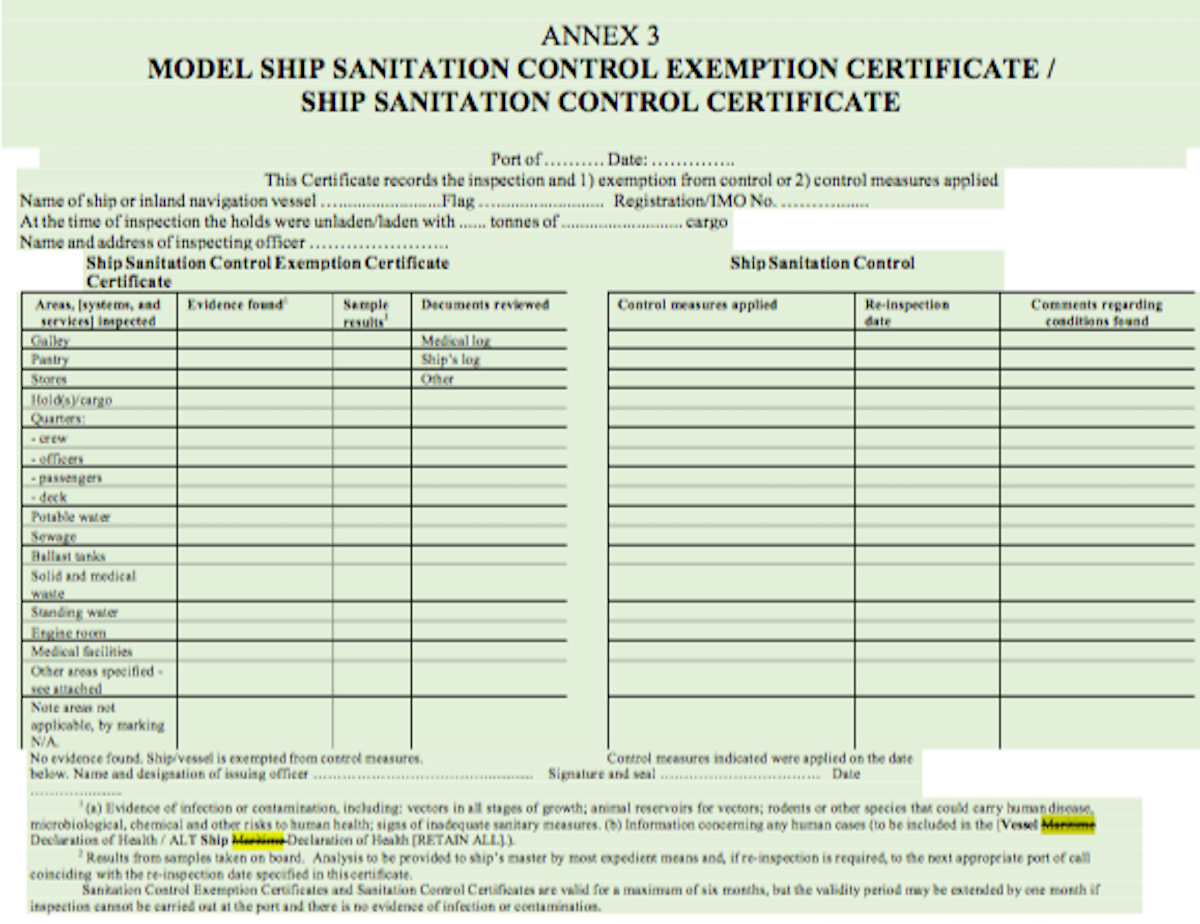
ANNEX 3:
ANNEX 4: TECHNICAL REQUIREMENTS PERTAINING TO CONVEYANCES AND CONVEYANCE OPERATORS
1. Conveyance operators shall facilitate:
(c) application of other health measures under these Regulations, including by providing conveyances with a plan to address situations where there is evidence of a public health risk on board as well as during embarkation and disembarkation;
ANNEX 6: VACCINATION, PROPHYLAXIS AND RELATED CERTIFICATES
1. Vaccines or other prophylaxis specified in Annex 7 or recommended under these Regulations shall be of suitable quality; those vaccines and prophylaxis designated by WHO shall be prequalified or listed for emergency use by WHO.
3. Certificates under this Annex are valid only if the vaccine or prophylaxis used has been prequalified or listed for emergency use by WHO.
4 bis. In accordance with Article 35, certificates, regardless of the format in which they have been issued, shall include elements allowing for the ascertainment of the certificate’s authenticity through non-digital means. This requirement shall be reviewed by the States Parties, based on developments, with a view to its modification as appropriate, at the Eighty-second World Health Assembly and shall conform with technical guidance and specifications in line with Articles 35 and 45. Without prejudice to the foregoing, certificates may also include additional elements allowing for the digital ascertainment of the certificate’s authenticity.
This certificate is valid only if the vaccine or prophylaxis used has been approved prequalified or listed for emergency use by the World Health Organization
Bureau’s text suggestion for “pre-qualification” raises concerns of vaccine supply concentration
The proposal states:
“Certificates under this Annex are valid only if the vaccine or prophylaxis used has been prequalified or listed for emergency use
approvedby WHO”.[The words in bold indicate the proposed text addition, and those in strikethrough are proposed for deletion].
The proposal to introduce these phrases came from the United States during the December 2023 meeting.
This amendment, if adopted, will make it compulsory to use only vaccines or prophylaxis that are WHO prequalified or listed for emergency use by WHO to issue vaccine/prophylaxis-related certificates.
ANNEX 7:
No amendments have been proposed to Annex 7. The current text from the International Health Regulations is included here for convenience.
REQUIREMENTS CONCERNING VACCINATION OR PROPHYLAXIS FOR SPECIFIC DISEASES
1. In addition to any recommendation concerning vaccination or prophylaxis, the following diseases are those specifically designated under these Regulations for which proof of vaccination or prophylaxis may be required for travellers as a condition of entry to a State Party:
Vaccination against yellow fever.
2. Recommendations and requirements for vaccination against yellow fever:
(a) For the purpose of this Annex:
(i) the incubation period of yellow fever is six days;
(ii) yellow fever vaccines approved by WHO provide protection against infection
starting 10 days following the administration of the vaccine;
(iii) this protection continues for the life of the person vaccinated; and
(iv) the validity of a certificate of vaccination against yellow fever shall extend for the
life of the person vaccinated, beginning 10 days after the date of vaccination.
(b) Vaccination against yellow fever may be required of any traveller leaving an area where the Organization has determined that a risk of yellow fever transmission is present.
(c) If a traveller is in possession of a certificate of vaccination against yellow fever which is not yet valid, the traveller may be permitted to depart, but the provisions of paragraph 2(h) of this Annex may be applied on arrival.
(d) A traveller in possession of a valid certificate of vaccination against yellow fever shall not be treated as suspect, even if coming from an area where the Organization has determined that a risk of yellow fever transmission is present.
(e) In accordance with paragraph 1 of Annex 6 the yellow fever vaccine used must be approved by the Organization.
(f) States Parties shall designate specific yellow fever vaccination centres within their territories in order to ensure the quality and safety of the procedures and materials employed.
(g) Every person employed at a point of entry in an area where the Organization has determined that a risk of yellow fever transmission is present, and every member of the crew of a conveyance using any such point of entry, shall be in possession of a valid certificate of vaccination against yellow fever.
(h) A State Party, in whose territory vectors of yellow fever are present, may require a traveller from an area where the Organization has determined that a risk of yellow fever transmission is present, who is unable to produce a valid certificate of vaccination against yellow fever, to be quarantined until the certificate becomes valid, or until a period of not more than six days, reckoned from the date of last possible exposure to infection, has elapsed, whichever occurs first.
(i) Travellers who possess an exemption from yellow fever vaccination, signed by an authorized medical officer or an authorized health worker, may nevertheless be allowed entry, subject to the provisions of the foregoing paragraph of this Annex and to being provided with information regarding protection from yellow fever vectors. Should the travellers not be quarantined, they may be required to report any feverish or other symptoms to the competent authority and be placed under surveillance.
ANNEX 8:
Please realize that the information in the above document is incomplete. The document makes no mention of the following:
- Article 2
- Article 3
- Article 13A
- Article 44A
- Article 53A
- Article 53 bis-quater
- Article 54
- Article 54 bis
- Annex 10
Please note that Articles 13A, 44A and Annex 10 were NOT included in the updated amendments above.
The Working Group for amendments to the International Health Regulations had a super-secret meeting on March 8, 2024. There were scheduled to discuss Articles 13A, 44A and Annex 10.
All they revealed to the public was 20 minutes of nothing…
WHY THE SECRECY?